Apollo College of Pharmacy, Durg 491001 (C.G), India
Two or more incidents within a six-month period or three or more within a year are considered recurrent urinary tract infections (rUTIs). With the exception of the first year of life, men to get urinary tract infections. UTIs cost the healthcare system a lot of money and cause many missed workdays. Antibiotics were once the mainstay of acute therapy; now, due to rising resistance patterns, antibiotic overuse and misuse, and a move toward antimicrobial stewardship, we are now depending increasingly on non-antibiotic and preventative measures. These are called recurrent UTIs. If they're not treated, recurrent UTIs can cause kidney damage, especially in kids younger than 6 , Berberine is the best herb for use the treatment of recurrent UTI. That are found in various plants such as European barberry and Oregon grape and the best source berberine in berberis aquifolium, that are belongs to the family of berberidaceae. Berberine is an important drug against many bacteria and combat infections by preventing the bacteria (E. coli and Proteus species) from adhering to the host cell. In this disease most common bacterial pathogen are Escherichia coli. Their treatment method are similar as the UTI. Recently cases of recurrent UTI in India 13%-14% of men will experience at least one
UTI (Urinary tract infection): An infection that affects a portion of the urinary tract is known as a urinary tract infection (UTI) (AL, 2013). While upper urinary tract infections (pyelonephritis) damage the kidney, lower urinary tract infections (cystitis) might affect the bladder or urethra. Suprapubic pain, painful urination (dysuria), and frequent and urgent urination even when the bladder is empty are signs of a lower urinary tract infection. On the other hand, kidney infection symptoms are more systemic and typically involve flank discomfort or fever in addition to lower urinary tract infection symptoms. Rarely, blood may be seen in the urine. At the extremes of age (i.e., in individuals who are very young or old), symptoms may be ambiguous or nonspecific. (AL, 2013) (Lane DR, august 2011)
Classification: The UTI classified as two types:
1. Uncomplicated UTI
2. Complicated UTI
Uncomplicated UTI: Uncomplicated UTIs also only occur due to specific bacteria, which are behind the vast majority of cases. The urethra and bladder are also known as the lower urinary tract. Some may refer to UTIs affecting the bladder as bladder infections or cystitis. Bladder infections are the most common Trusted Source form of UTI. (Salvatore S, june2011)
Causes: Bacteria strains that could cause uncomplicated UTIs include:
E. coli and Klebsiella cause the vast majority Trusted Source of uncomplicated UTIs.
Complicated UTI: A complicated UTI is any urinary tract infection that does not fit the criteria of an uncomplicated UTI. If a doctor thinks that the UTI will be difficult to treat or could lead to complications, they will define it as a complicated UTI. (Salvatore S, june2011) A UTI can also be a complicated case if the bacteria that cause it are ones that do not typically cause UTIs.
Causes: The same bacteria that cause uncomplicated UTIs can also cause complicated UTIs. A range of different microbes can also cause complicated UTIs. This includes different bacteria and, in some cases, fungi such as Candida. Some bacteria that cause complicated UTIs may be resistant to antibiotic treatment. (Chae JH, november2015)
Sign & symptoms:
Bladder infections are another name for lower urinary tract infections. The most typical symptoms include burning when urinating, frequent urination (or the need to urinate) without vaginal discharge, and severe pain. In healthy women, these symptoms typically last six days and can range in severity from mild to severe. (Salvatore S, june2011)It's possible to have some lower back or pubic bone ache. In addition to the typical symptoms of a lower urinary tract infection, people with pyelonephritis, or upper urinary tract infection, may also have fever, nausea, and vomiting, or flank discomfort. Rarely, there may be visible pus in the urine or it may seem bloody. (Chae JH, november2015) UTIs have been associated with onset or worsening of delirium, dementia, and neuropsychiatric disorders such as depression and psychosis. However, there is insufficient evidence to determine whether UTI causes confusion (Krinitski D, (November 2021) .The reasons for this are unknown, but may involve a UTI-mediated systemic inflammatory response which affects the brain. Cytokines such as interleukin-6 produced as part of the inflammatory response may produce neuroinflammation, in turn affecting dopaminergic and/or glutamatergic neurotransmission as well as brain glucose metabolism. (Lane DR, august 2011)
Recurrent UTI (rUTI):
rUTIs are prevalent and pose a serious threat to public health and society. Both the lower and upper urinary tracts may be affected, but if upper UTIs recur frequently, a complex aetiology should be suspected. (O'Riordan, May 2023) Antibiotics have undeniable therapeutic benefits, but because of their extensive use, urinary tract infections have become more resistant. Between 20% and 50% of antibiotic prescriptions in acute hospital treatment are thought to be either unneeded or inappropriate. The goal of antimicrobial stewardship is to mitigate the consequences of these pervasive prescribing practices. (O'Riordan, May 2023) While reducing the negative impacts of antibiotic use, such as toxicity, the selection of aggressive organisms, the rise of resistant bacterial strains, and healthcare-associated infections like Clostridium difficile, it seeks to enhance therapeutic outcomes and guarantee cost-effective therapy. (a, February 2005) The WHO has declared that antimicrobial resistance (AMR) is one of the top ten global public health threats facing humanity and has developed a global action plan for AMR. (Krinitski D, (November 2021) As a result of the adherence to these principles, there is now increased interest and use of non-antibiotic adjuncts in the treatment and prophylaxis of UTIs. (O'Riordan, May 2023)
Sign and symptoms:
Symptoms of a recurrent urinary tract infection (UTI) include:
Chronic UTIs can lead to serious complications, including kidney infections, kidney disease, sepsis, and premature delivery.
In infants and young children, signs of a UTI may be nonspecific, such as fever, vomiting, or decreased appetite or activity. Some factors that can contribute to recurrent UTIs in females include: E. coli bacteria from the rectal bacterial flora, Sexual activity, Spermicide use, and Menopause.
Dignosis:
rUTIs are recurrences of uncomplicated and/or complicated UTIs (see Table 1). The spectrum of UTI ranges from self-limiting cystitis with mild symptoms to life-threatening sepsis and Fournier's gangrene (Jiang Z, September 2022). Even when mild, they can account for morbidity for the patient and account for significant time off work and regular duties. Initial diagnosis of a lower urinary tract infection is normally made clinically, with the patient presenting with features, such as new urgency, frequency, dysuria. (Amdekar S, nov2011)
Differential diagnoses:
The differential diagnosis can be determined by the patient's age and sex. Younger patients should be worked up for sexually transmitted infections (STIs) such as gonorrhoea and chlamydia. Women of child-bearing age should be considered for bacterial vaginosis and candida. Older patients are more at risk for lichen sclerosis et atrophicus and the genitourinary syndrome of menopause (formerly known as vulvo-vaginal atrophy) in postmenopausal women. (Jiang Z, September 2022)
Aetiology:
Bacterial infection accounts for most UTIs, however viral and fungal infections can also occur, particularly in the immunosuppressed. The most common bacterial pathogen is Escherichia coli. Other common pathogens include Klebsiella pneumoniae, enterococcus faecalis, proteus mirabilis and pseudomonas aeruginosa (O'Riordan, May 2023). Most Gram-negative bacteria arise from the gastrointestinal tract and ascend via the urethra. It is rarer for UTI to occur as a result of haematogenous spread.
Pathogens:
The distribution of microbes in the three urine cultures necessary for the rUTI diagnosis is shown in Figure 1, the most common being Escherichia coli (41%) (O'Riordan, May 2023).
Risk Factor:
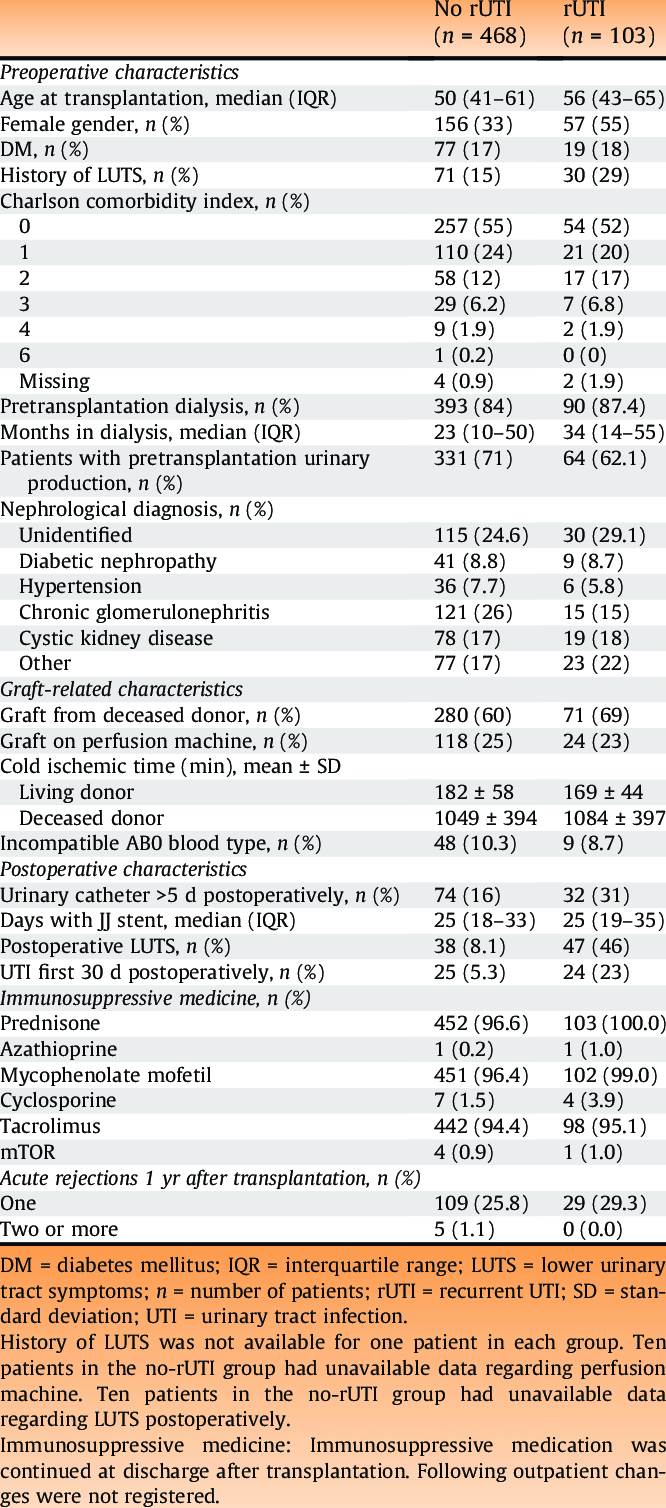
In a multivariable analysis, increasing age, female gender, and a preoperative history of lower urinary tract symptoms were significantly associated with rUTIs compared with the rest of the transplant recipients . Experiencing a UTI within the first 30 d postoperatively was the risk factor that had a strong association with an rUTI, with the highest hazard ratio. Pretransplantation urinary production, defined as <100>

Fig. 1 – Frequency of microbe groups found in the three diagnostic urine cultures for rUTI. The numbers in bars represent the absolute numbers. rUTI = recurrent urinary tract infection; UTI = urinary tract infection.
Some risk factors for recurrent urinary tract infections (UTIs) in men include:
Table 1 – Clinical characteristics of the cohort, stratified for patients with or without rUTIs
Treatment strategies for managing recurrent UTIs:
Strategies include behavioural modifications, such as avoidance of risk factors; non-antibiotic options and antibiotic options.
Behavioural modifications are commonly recommended but these practices are not strongly supported by evidence. It is known that sexually active women and those who use spermicides are more likely to be at risk of a UTI. Behavioural modifications can play a role here. Other recommendations, although likely apocryphal, include optimizing diabetic control, timed voiding, avoidance of diaphragm use, post-coital voiding, wiping from front to back after defaecation and the wearing of cotton. (O'Riordan, May 2023)
Post-menopausal women tend to develop changes to their oestrogen-sensitive tissues such as the vulva, vagina and urethra. This can lead to a reduction in host factors which protect against UTI. The epithelium thins, tends to crack, loses elasticity and becomes dry, the pH rises, the numbers of normal commensal lactobacilli diminish, leading to an overgrowth in pathogenic bacteria. This is called the genitourinary syndrome of menopause (GSM) (formerly vulvovaginal atrophy) (O'Riordan, May 2023).
Treatment and further examination:
In the rUTI patient group, 39 (38%) were started on prophylactic antibiotic treatment after the rUTI diagnosis to prevent further UTIs. The most used were pivmecillinam (64%), trimethoprim (15%), nitrofurantoin (7.7%), and ciprofloxacin (7.7%). Local estrogen was given to 22 (39%) of female recipients as a prophylactic measure for rUTIs. (b, June 2023) A total of 57 of 103 patients were referred for a urological workup for further examination of their underlying pathophysiology. Male patients (33 of 46) with rUTIs were referred to a urologist more often than females (24 of 57). Fifteen of 57 female recipients with rUTIs were referred to a gynecologist. (O'Riordan, May 2023) Thirty of the total 57 female recipients with rUTIs were referred to a urologist and/or gynecologist, and some were referred to both.
The urological examinations included cystoscopy (79%), flow and residual urine test (71%), computed tomographic urography (32%), and urodynamic test (21%). Urological workup resulted in a diagnosis of 26 patients, of whom 16 (28%) were diagnosed with residual urine although no strict definition was used, five (8.8%) with benign prostatic hyperplasia, two (3.5%) with urethral stricture, two (3.5%). (b, June 2023)
Antibiotic choice is guided by:
There are many patent factors which need to be taken into consideration when prescribing antibiotics. These include drug allergies, renal/hepatic function, presence of interacting drugs, comorbidities, age, pregnancy and host-immune function (b, June 2023).
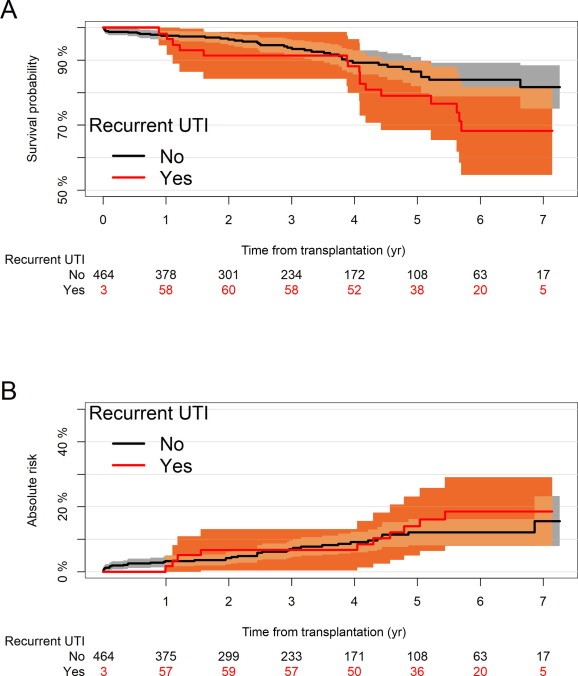
Fig. 2 – (A) Cumulative incidence of graft loss, with death as a competing risk. (B) Kaplan-Meier plot on overall patient survival comparing patients having rUTI with those having no rUTI. The analysis is adjusted for the immortality bias by delayed entry in the recurrent UTI group. Be aware that the Y axis shows a limit of 50%. rUTI = recurrent urinary tract infection; UTI = urinary tract infection.
Treatment method for recurrent UTI (rUTI):
Treatment method for recurrent urinary tract infections (UTIs) can include:
Some other tips to prevent UTIs include: Wiping from front to back, Urinating before and after sex, Drinking lots of water, and Avoiding tight underpants and jeans (AL, 2013).
Drugs used in treatment of recurrent UTI:
Antibiotics are commonly used to treat urinary tract infections (UTIs) in men, and the preferred drugs for recurrent UTIs include:
Other antibiotics used to treat UTIs include:
Adult men with UTIs should take antibiotics for 10–14 days. Phenazopyridine can be used to treat the symptom of dysuria (Chae JH, november2015).
Carbapenems are another type of antibiotic that are often considered a drug of last resort. Common side effects include nausea and vomiting. At high doses, these drugs can cause seizures, especially imipenem (AL, 2013).
Herbal Medicines (Phytoconstituent):
Berberine is an important drug against many bacteria and combat infections by preventing the bacteria (E. coli and Proteus species) from adhering to the host cell, which suggests their potent role in treating rUTI. Berberine, a compound found in various plants, such as European barberry and Oregon grape, has a long history of medicinal use dating back over 3,000 years. It has potential benefits in treating conditions such as recurrent UTI, diabetes, high cholesterol etc.
Berberine dosage
The suggested dose of berberine is 250 milligrams or 500 milligrams two or three times a day.
Management of recurrent UTI (rUTI):
Recurrent urinary tract infections (rUTIs) can be managed with a combination of behavioral changes, antibiotics, and other treatments:
For women with cystitis associated with sexual activity, postcoital antibiotics can be taken to reduce the risk of adverse effects. For other cases, continuous prophylaxis may be recommended. Some common antibiotics used for prophylaxis include Bactrim, Fosfomycin, and Nitrofurantoin.
Some studies have shown that cranberry juice or tablets can reduce the number of symptomatic UTIs over a 12-month period. However, other studies have found that cranberry juice is not effective in preventing rUTIs.
This can be recommended for postmenopausal women with vulvovaginal atrophy.
Patients with a PVR volume greater than 50–100 mL may benefit from conservative measures to reduce PVR, such as pelvic floor exercises or relaxation techniques.
These include drinking at least 2 liters of fluids per day, wiping from front to back, and avoiding reusable sponges and luffas.
Some patients may need to be referred to a urologist for further investigation or other treatment strategies.
Surgical management:
Urethral dilatation is a traditional treatment for prevention of rUTI although it lacks robust evidence. Future therapies may involve the use of intravaginal laser in an attempt to replenish normal vaginal defences by boosting collagen production. Some patients may need to be referred to a urologist for further investigation or other treatment strategies.
Cases of recurrent UTI in MEN in India:
Although recurrent UTIs are more common in women, around 20% of all diagnosed UTI cases occur in men. Despite the lower incidence, approximately 13–14% of men will experience at least one UTI in their lifetime, compared to around 50% of women (Sarita Mohapatra 1, 2022 Feb ).
CONCLUSION:
Preventing rUTIs is probably an unattainable goal. Instead, our focus should be on reducing the number of recurrent UTIs and morbidity associated with them. Our armamentarium has expanded exponentially and the single-pronged approach of treatment dose-antibiotics is now something of the past. Patients and clinicians now have several strategies to reduce the recurrence of UTIs ranging from behavioural modifications, non-antibiotic treatments and different regimens of antibiotic treatments. One in six patients experience rUTIs after RTx. Pre- and postoperative variables affect the risk of rUTIs, but none are easily modifiable. In this cohort, rUTIs did not affect the graft function or survival. The etiology of rUTIs remains poorly understood, and there is a continuous need to study how rUTIs can be reduced and treated optimally. There are several risk factors that can guide early detection and management. We could not demonstrate an effect of rUTIs on graft or patient survival. Also in this cohort, but is not necessarily different from the background population. Besides the above statistical result-based conclusions, this complex UTI clinic service also reinforced that clinical history is crucial and exploring the drug allergies to assess their severity is vital to not miss out on potential treatment options through a risk versus benefit analysis. MDT approach (involving the microbiologists) adds a different perspective and dimension to management
REFERENCE





Guman, Hari Prasad Sonwani*, Shweta Kumar Saw, Upasana Sahu, Jayvant Kumar Sahu, Yunesh Kumar Mandavi, Recurrent UTI in MEN: Risk Factor and Management: a review, Int. J. Sci. R. Tech., 2025, 2 (2), 87-95. https://doi.org/10.5281/zenodo.14846234
 10.5281/zenodo.14846234
10.5281/zenodo.14846234
