
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Rashtriya College Of Pharmacy Hatnoor Tq.Kannad Dist.Chh.Sambhajinagar,Maharashtra,India-431103
Nanoemulsions are considered as the most promising solution to improve the delivery of ophthalmic drugs. The design of ophthalmic nanoemulsions requires an extensive understanding of pharmaceutical as well as technological aspects related to the selection of excipients and formulation processes. This Review aims at providing the readers with a comprehensive summary of possible compositions of nanoemulsions, methods for their formulation (both laboratory and industrial), and differences between technological approaches, along with an extensive outline of the research methods enabling the confirmation of in vitro properties, pharmaceutical performance, and biological activity of the obtained product. The composition of the formulation has a major influence on the properties of the final product obtained with low-energy emulsification methods. Increasing interest in high-energy emulsification methods is a consequence of their scalability important from the industrial perspective. Considering the high-energy emulsification methods, both the composition and conditions of the process (e.g., device power level, pressure, temperature, homogenization time, or number of cycles) are important for the properties and stability of nanoemulsions. It is advisible to determine the effect of each parameter on the quality of the product to establish the optimal process parameters? range which, in turn, results in a more reproducible and efficient production.
Basic information of nanoemulsions
Nanoemulsions are a type of emulsion where two or more immiscible liquids are mixed together and stabilized withsurfactants or emulsifiers. The resulting droplets have adiameter of less than 1000 nanometers (nm). A nanoemulsion is a type of emulsion where two or more immiscible liquids are mixed together and stabilized with surfactants or emulsifiers1. The resulting droplets have a diameter of less than 1000 nanometers (nm).In simpler terms, a nanoemulsion is a mixture of two or more liquids that don't normally mix, like oil and water, blended together in a way that creates tiny droplets that are stable and don't separate
Oil-in-water (O/W): Oil droplets dispersed in a water phase.Water-in-oil (W/O): Water droplets dispersed in an oil phase.2Depending on constituents and relative distribution of the internal dispersed phase/phases and the more ubiquitous continuous phase, nanoemulsions are termed as biphasic (O/W or W/O) or multiple nanoemulsions (W/O/W). Phase volume ratio (?) measures comparative volumes of internal and external phase comprising a nanoemulsion and determines its droplet.number and overall stability. Normally, phase present in greater volume becomes the external phase. To predict type of nanoemulsion formed under
Ophthalmic: Targeted delivery of medications to the eye.
larger cavitation zones; therefore, they process much more material per unit of time as compared with laboratory sonicators. Furthermore, scaling-up the process requires the samecavitation intensity in the production environment as originally used in the laboratory. It means that to obtain reproducible results after scale-up, the sonotrode amplitudes in laboratory and industrial processors must be kept at the same level. Conventional industrial ultrasonic devices cannot provide high enough amplitudes for efficient nanoemulsification that compromise the product quality. Newly developed industrial ultrasonic devices that utylise so-called Barbell Horn Ultrasonic Technology (BHUT) provide the same high ultrasonic amplitudes and cavitation intensity as used during the laboratory phase of product development, enabling the achievement of reproducible results on an industrial scale.
The increased ability to solubilize the sparingly soluble active substance in nanoemulsions results in longer release of an API from these systems, as compared with conventional drug forms (e.g., eye drops), enabling the achievement of the therapeutic effect using a lower dose of the drug and to decrease the number of systemic side effects9.The in vitro release study of the API from nanoemulsions allows determination of the release kinetics of the drug from a given formulation, which may provide preclinical data on the biodistribution and bioavailability of the drug into the eye. Sustained release formulations may provide the drug penetration into the deeper layers of the eye structure after application. Biorelevant methods of testing the release of ophthalmic products in vitro are still under development. Since there are no accepted compendial standards for this area we provide the overview of different noncompendial methods used for evaluation of drug release from ophthalmic nanoemulsions in this section10. In vitro drug release from these systems is currently being assessed using a variety of membrane diffusion techniques including simple dialysis methods, dialysis methods using a modified type I or II apparatus, and Franz diffusion cells. The aforementioned USP type II apparatus is preferred for testing the release of substances from ophthalmic nanoemulsions. In this method, the formulation (0.5 mL) is placed in a dialysis bag and installed in the beaker containing an acceptor medium. The release test is usually performed at 34 ? 0.5 ?C or 37 ? 0.5 ?C in 900 mL of phosphate buffer at pH 7.4, often with addition of 1% sodium lauryl sulfate (SLS) or a buffered saline solution (PBS) at pH 7.4 with rotational speed of blades set to 50 rpm. The test is carried out in 3 replications for 6 h11. The medium samples are withdrawn at specified intervals and the loss of the collected medium is replenished with a fresh buffer in order to maintain a constant fluid volume. The concentration of the active substance is determined using high-performance liquid chromatography (HPLC) or UV?vis spectroscopy.
During the release of the API from nanoemulsion, the drug diffuses from the oil droplets into the surrounding aqueous environment. Depending on its solubility and the volume of the aqueous environment, the drug may dissolve or precipitate, which may lead to unreliable results. The method utilizing the type II apparatus can be used in the study of the release of substances from nanoemulsions when the concentration of the substance in the formulation exceeds its water solubility. Moreover, the large volume of the dissolution medium can help overcome the difficulties in maintaining sink conditions for poorly soluble drugs. In vitro drug release studies using membrane-free diffusion methods have also been described. However, because of the direct contact of the tested systems with the dissolution medium, their possible aggregation and/or disintegration in the dissolution medium should be assessed. In vitro drug release experiments are typically conducted under sink conditions which can be achieved with a relatively large volume of dissolution medium (i.e., from 40 to 200 mL). It can be expected that the small volume of the dissolution medium more accurately reflects the in vivo conditions since the average amount of tear fluid produced in the precorneal area during the 24 h period is 2 mL. However, in an in vitro drug release study from contact lenses, it has been shown that small volumes of dissolution medium are not suitable for in vitro testing or do not reflect the precorneal environment.In order to minimize the effects of the unstirred aqueous layer, in vitro drug release experiments are performed at different agitation rates; for example, from 20 to 100 rpm for dialysis methods using a paddle dissolution apparatus, to 150 and 600 rpm for simple dialysis and Franz diffusion cell methods. Drug release studies are also performed using vertical Franz diffusion cells with an effective area of 1.13 cm2 into simulated tear fluid at pH 7.4. The nanoemulsion (1 mL) is deposited onto the previously soaked dialysis membrane which separates the donor and acceptor chambers, taking samples at regular intervals and replacing them with the same volume of fresh medium.It should be stressed that sink conditions in the eye can be maintained if the drug clearance is high. However, the total clearance mechanism (including lacrimal turnover and absorption by the conjunctiva) is complex and difficult to simulate in in vitro studies. In physiological conditions the human eye contains a tear volume that ranges from 6.2 to 30.0 ?L and the tear flow rate assumes values between 0.9 and 2.1 ?L/min. In order to predict the drug release kinetics in the eye in a more reliable way , it is crucial to develop microfluidic models that mimic the hydrodynamic conditions of the eye as accurate as possible.
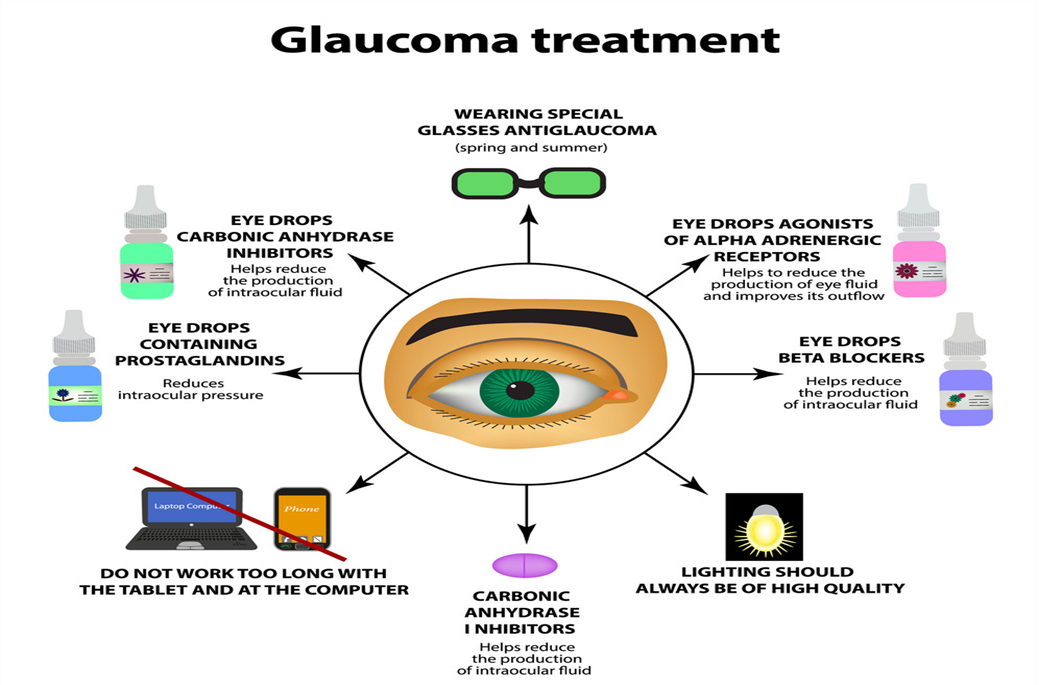
The current objective of glaucoma treatment are to prevent damage to the optic nerve, preserve the patient s visual field, and mamitaintheire quality of life by minimizing the side effect of medication of the several factor that might increase the risk of glaucoma development, IOP is considered the most crucial and omly practicable risk factor of glaucoma IOP? reduction inhibits the progression of glaucoma Threfore, it is essential to prioritize IOP the therpy consists of applying antiglucoma eye drops directly to the affected area, followed by the administration of oral drug, lasur treatment, and surgery if necessary. The treatment of glaucoma can be categorized into medical therpy, lasaretherapy and surgery 15Topical eye drop of antiglucoma drugs effectively reduced the IOP and several therapeutic agent with specific mechanism are used for ex, cholinergic agonists stimulnate the contraction of the ciliry muscle, leading to a more spherical shape of the lense and an increase muscle, leading to a more spherical shape of the lenses and an increase in theire focusing ability, and also contracted the cells of the lences and increses in theire focusing ability, and also conttraced the cell of trabecular meshwork [TM].
? ? ? ?
? ? ? ? ? ? 
? ? ? ?
? ??
? ? ? ?
? ? ? ? ? ? 
? ? ? ?
16The surface of the eye after a single blink of eye, and almost all administered formulation is cleared from the eye surface within 15-25 min allowing a short duration of about 5-7 min for absorpation of administered drug eventually around 5% of topically administered formulation may overawed the barrires and reached is required, which lesds to patimt incompliance and early termination of medication these ocular barrirs also play a role in the fluctuating threpeutic effect that occurs before and after each appalication of the eye drops the variation in medication concentration over time might cause fluctuations in IOP at various times intervals of the day which is likely to contribute to the development of glaucoma Sometime ,medical therpy may not effectively reduce the IOP to the desired levels, despite the use of the most effectively medications for management of glaucoma, the use disease may still progress and lead to the degradation of the optic nerve in such cause,trabeculoplasty may be investigated as a treatment option to decrease IOP in patint with open-angle glaucoma argon laser trabecuoplasty (ALT) involve targeting the TM cells carrying pigment with laser triggering coagulative necrosis as well as thermal damage which induce the contraction of the TM hence increasing the drainage capacity of the aqueushumor the argon lasae harms extends beyond the target region containing melanin protin. The use of ALT might result in significant advers effects, including peripheral anterior anterior synechiae, uveitis and temporary icreases in IOP conversely Q-swithched Nd: YAG laser with double frequency is used for the purpose of selective laser trabecuplastry (SLT) decreases IOP by various mechanism, including the stimulation of and extracellular matrix synthesis and turnover, displacement of cell extraction matrix (ECM) synthesis
? ? ? ?
? ? ? ? ? ? 
? ? ? ?
The idea of nanocarrires was first introduced in 1980s; however the word nanomedicine was first officially definds by european science foundation (ESF) in 2003.17Finally, in 2010 the precise definition of nanomedicine was established as the extentesive monitoring regulate construction repaire, defence and enhacement of biological system of human at molecular level with help of engineered nanostructures and nanodevices operating single-cell level with the ultimate goal of achievices enhanced therapeutic benefits nanomedicines,a branch of nanotechnology, playa significant role in the diagnosis and treatment of various disease including ocular diseases by greatly enhacing the efficacy of therepics. Nanomedicine has the capacity to encapsulate a wide range of therapeutic ?agent. 18The enacasulation of drug molecule in nanomedicine proteck them from degradation and also inhance the targeting ability via surface modification significant effectively to anteriorsegment of eye. Chitosan (CH), hydroxypropyl methylecellulose(HPMC), gellangelatin, hyaluronic acid(HA), and carboxmethlcellulose are often used as a mucoadhesive agets in the formulation nanomedicines to extend the retention time on ocular surface and may show resistance to ocular clearance as a result of the movement of blinling and the impulsive production of tears. Furthermore, the outermost layer of the cornea, know as the superficial corneal epithelium, is coated with a mucin membrane that carries a negative charge thise creates an ideal surface for attachaing nanocarriers that have a positive charge
Case studies of nanomedicine for glaucoma treatment
|
Drug |
Dosage |
Application/Advantages |
|
Timolol |
Contact lenses |
Bioavailability enhancement |
|
Dorzolamide |
Drops |
Increased corneal penetration Ability, prolonged drug action Time with sustained drug |
|
Pilocarpine |
Drops |
Poolonged drug action time With sustained drug relese |
|
Travoprot |
Drops |
Increased corneal penetration Abiity. |
|
Timolol |
Drops |
Enhanced corneal permeati- -on ability. |
|
Noisome |
Gels |
Prolonged drug action time With sustained drug relese |
|
Timolol |
Gel |
Prolonged drug action time With sustained drug relese |
?
Ophthalmic o/w nanoemulsions can generally be considered as dispersions of oily droplets in an aqueous environment. Therefore, these formulations require careful selection of the composition of both the oily phase (i.e., the use of nontoxic, nonirritating, pharmaceutically approved oils) as well as the composition of the aqueous medium . Similarly to the ophthalmic drops the need for isotonicity of the ocular nanoemulsions, the desired pH, a certain buffering capacity, the addition of preservatives (antimicrobial agents), viscosity modifiers, and antioxidants calls for careful consideration19. Furthermore, in order to obtain nanosize uniform droplets of oils, an extensive optimization of the composition as well as the concentration of surfactants and cosurfactants in the formulation are required. The complexity of ophthalmic nanoemulsion compositions demands comprehensive knowledge and experience in pharmaceutical formulations so stable products of pharmaceutical quality couldbe designed. In this section we provide detailed characteristics of the most frequently used components of ophthalmic nanoemulsions including oils, emulsifiers, surfactants, and cosurfactants as well as additives used to modify their pharmaceutical properties (e.g., tonicity, viscosity, or pH of the formulation
Ophthalmic nanoemulsions contain from 5 to 20 wt % of oil/lipid as the dispersed phase. The selection of the lipid phase is an important aspect in the design of nanoemulsions, as API is dissolved in an oil prior to the dispersion in an aqueous phase. The selection of the oil phase for nanoemulsion formulation is frequently based on the solubility of API in different oils.9 In addition, the oil used in the formulation needs to be well tolerated and compatible with the other excipients included in the nanoemulsion. The following compounds are frequently used to prepare ophthalmic nanoemulsions vegetable oils, glycerides, medium-chain triglycerides, long-chain unsaturated fatty acids, and polyalcoholic esters of medium-chain fatty acids20. Vegetable oils administered topically to the eye include: soybean oil, castor oil, peanut oil, olive oil, jojoba oil, and Babchi seed oil.Medium-chain triglycerides such as Miglyol 812, Captex 355, 200 or 8000, Witepsol, and Labrafac as well as long-chain unsaturated fatty acids (oleic and octanoic acids) are also used as an inner phase of nanoemulsions. From the group of polyalcoholic medium-chain and long-chain fatty acid esters, the following are used: ethyl oleate, isopropyl myristate and isopropyl palmitate. Triacetin and vitamin E are also mentioned among the ingredients of the nanoemulsion applied to the eye, and additionally, these two compounds in ophthalmic formulations can act as humectants and antioxidants.
21The form of nanoemulsion for ophthalmic drug delivery system for treating several eye diseases like dry eye syndrome, glauco.Several drugs are formulated in ma, etc . A combination of oil in water type emulsions are being generated usually for improved topical lipophilic drug delivery to the eye. Lipophilic drug is usually having increased absorptivity compared to lipophobic. The bioavailability is enhanced, and the patient compliance is found to be better when nanoemulsion are topical
Nanoemulsinsare extensively used in pharmaceutical dosage forms for delivery of drugs to eye, which proposes several benefits such asNanoemulsi delivery of medications, biological or analytical agents. The most significant application of ophthalmic nanoemulsion is longer residence time in the eye cavity and larger bioavailability in comparison with the conventional drug delivery systems like eye drop solutions and suspensions. Ophthalmic nanoemulsions may also deliver the drugs, which are prone to hydrolysis and oxidation overall all ophthalmic nanoemulsion preparation by be considered as active safe and with superior bioavilability it is predictable that additional research and development will be conduced out in the future concerning ophalmic nanoemulsion.
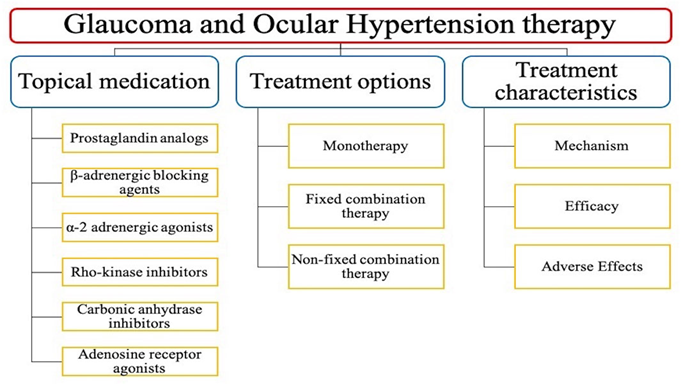
Classification of glaucoma treatment
? ? ? ?
? ? ? ? ? ? 
? ? ? ? ??
1.???????????????????? Timolol maleate; A beta-blocker used to reduce intraocular pressure.
2.?????????????? Pilocarpine; A muscarinic recptor agonist used to reduce intraocular pressure.
3.?????????????????? Latanoprost;A prostaglandin analogusedto reduce intraocular pressure.
4.???????????? Brimonidine; An alpha-2 adrenergic agonist used to reduce intraocular pressure.
Timolot maleate
The maleate salt form of timolol, a propanolamine derivative and a non-selective beta-adrenergic antagonist with antihypertensive property. 22Timolol competitively binds to beta-1-adrenergic receptors in the heart and vascular smooth muscle and beta-2-receptors in the bronchial and vascular smooth muscle, resulting in a decrease in beta-adrenergic stimulation. Beta-1-receptor blockade results in a decrease in resting and exercise heart rate and cardiac output, a decrease in both systolic and diastolic blood pressure, and, possibly, a reduction in reflex orthostatic hypotension. Beta-2-blockade results in an increase in peripheral vascular resistance. The ultimate results include vasodilation, and negative chronotropic and inotropic effects. In addition, timolol reduces intra-ocular pressure possibly by decreasing aqueous humor production by reduction of blood flow to the ciliary processes and cAMP synthesis.Timolol is used in the treatment of ocular hypertension and glaucoma Timolol is a beta blocker. It works by decreasing the production of aqueous humour (fluid in the eye), thereby lowering the increased eye pressure
? ? ? ?
? ? ? ? ? ? 
? ? ? ?
?Machanishm Ction Of Timolol Maleate? In Gluacoma:
Open-Angle Glaucoma
The exact mechanism of action by which timolol reduces the intraocular pressure in patients with open-angle glaucoma is unknown. 21Timolol is thought to inhibit ?-receptors on the ciliary epithelium, which normally functions to increase the production of aqueous humor. Some researchers have proposed that by inhibiting these receptors, timolol reduces aqueous humor production and, therefore, reduces intraocular pressure.Researchers have also studied non-adrenergic pathways of timolol to reduce intraocular pressure.
Ocular Hypertension
Timolol's mechanism of action in reducing intraocular pressure in patients with ocular hypertension is unknown22. Still, it appears similar to its mechanism in lowering intraocular pressure for patients with open-angle glaucoma.
Infantile Hemangioma
Timolol is thought to antagonize ?-adrenergic receptors, causing multiple processes, including vasoconstriction, apoptosis stimulation, and angiogenesis inhibition.
Hypertension
The sympathetic nervous system is an essential component of blood pressure regulation. Usually, ?-1 and ?-2 receptors are activated by endogenous catecholamines. 23These activated receptors stimulate their associated G-protein, activating adenylyl cyclase and increasing cyclic-AMP (cAMP) levels.This secondary messenger initiates a cascade of reactions in the body, including vasoconstriction and elevated blood pressure. Nonselective ?-blockers (eg, timolol) block interactions between endogenous catecholamines and prevent the G-protein cascade from occurring, reducing sympathetic tone and decreasing blood pressure.
Myocardial Infarction
There are many mechanisms by which ?-blockers can reduce morbidity and mortality in patients after myocardial infarction. For example, ?-blockers can reduce myocardial oxygen demand and relieve ischemic chest pain. By blocking the sympathetic receptors in the heart, timolol decreases heart rate. This induced bradycardia prolongs diastole, allowing for increased perfusion of the heart.Beta-blockers can inhibit platelet aggregation and thromboxane synthesis and reduce the rate of atherosclerosis and thromboembolism. They also inhibit cardiac remodeling after myocardial infarction.
Migraine Prophylaxis
The exact mechanism of timolol for migraine prevention is unknown. One proposed mechanism involves the antagonism of ?-adrenergic receptors, which decreases the synthesis and release of norepinephrine, a key intermediate in the pathophysiology of migraines. Another mechanism that could explain timolol's migraine prophylactic properties is based on the ability of ?-blockers to regulate the neuronal firing of periaqueductal gray matter using gamma-aminobutyric acid (GABA)24,25. Timolol also appears to play a role in regulating the serotonergic system by inhibiting serotonin (5-HT), another important mediator in the pathophysiologic pathway of migraines26. This modulation of serotonin's effects seems to contribute to the ability of ?-blockers to reduce the sensitivity of the auditory system, reducing the frequency of migraine attacks. There is also a hypothesis that ?-blockers play a significant role in reducing the excitability of the visual system in patients with migraines. Beta-blockers such as timolol are also thought to reduce the spread of signals through the brain, including the cortical spread and the excitability of the ventroposteromedial thalamic nucleus.
Atrial Fibrillation
The autonomic nervous system plays a significant role in developing atrial fibrillation. Aberrant sympathetic tone can stimulate myocyte contraction and promote irregular rhythms in susceptible patients. Beta-blockers help maintain the heart's regular rhythm by decreasing the autonomic tone and, therefore, decreasing sympathetic stimulation of the cardiac myocytes.
CONCLUSION
The ophthalmic drug market has significantly grown in recent years globally. Between 2015 and 2018 there was an 800% increase in approvals of new ophthalmic drugs including topical treatments.118?120 Although manufacturers are increasingly investing in research and development of innovative, noninvasive ophthalmic preparations, there is still a significant unmet need for the availability of multiactive ophthalmic drug formulations, including combination therapy products. Formulation of complex innovative drug delivery systems, such as ophthalmic nanoemulsions, requires extensive understanding of pharmaceutical aspects related to the selection of auxiliary substances and quality control methods that guarantee the desired properties, stability, and tolerance of the formulation during shelf life and after its application. Furthermore, from a formulation scientists? perspective, it is of great importance to select robust optimizable technological processes enabling efficient manufacturing of ocular nanoemulsions on an industrial scale. This also includes formulation of sterile products as well as selection of packing and dosing devices. Ophthalmic nanoemulsions formulations require optimization of both composition and manufacturing methods. The optimization process involves several critical nanoemulsion properties, for example, particle size and its distribution,stability, contact time at the application site, and tolerance.The available research indicates that size of oil phase droplets is strongly affected by the nanoemulsion composition, manufacturing technique, and preparation conditions. Therefore, there is a need for continuous research enabling tounderstand the interplay between the composition of nanoemulsions, their preparation techniques, and properties of the formulation. Furthermore, successful implementation of the nanoemulsion-based formulations into medical practice requires a comprehensive evaluation of their quality using well-defined, standardized analytical methods, and research protocols. Despite the continued interest in nanoemulsions formulation with low-energy methods, a growing share of the use of high-energy methods is observed
REFERENCE


Avinash Gite*, Nikam.H.M, Pawan Hadole, Pratik Kamble, Umesh Jadhav, Ophthalmic Nanoemulsions: From Composition to Technological Processes and Quality Control, Int. J. Sci. R. Tech., 2025, 2 (1), 150-161. https://doi.org/10.5281/zenodo.14634480
 10.5281/zenodo.14634480
10.5281/zenodo.14634480