1Student, M Pharmacy Department of Pharmacy Practice, Al- Ameen College of Pharmacy, Bengaluru, India.
2Head of Department, Department of Pharmacy Practice, Al- Ameen College of Pharmacy, Bengaluru, India.
3Department of gastroenterology, St. Philomena’s Hospital, Bengaluru, India
Chronic liver disease (CLD) is a global health concern characterized by persistent liver dysfunction, leading to fibrosis and cirrhosis. This nine-month prospective observational study aimed to assess the risk factors, management, and health-related quality of life (HRQoL) in CLD patients. Conducted at St. Philomena’s Hospital, the study included 102 patients, aged 18 and above, with confirmed CLD diagnoses. Demographic, social, and medical data were collected, and HRQoL was assessed using the SF-36 questionnaire. The majority of patients were male (76.47%), aged 51-60 years (37.25%), with a significant history of alcohol consumption and comorbidities such as diabetes. Clinical manifestations like edema were common, and liver damage was indicated by abnormal liver function tests. Most patients received diuretics, hepatoprotective agents, and nutritional supplements. SF- 36 results revealed that most patients had a poor quality of life, highlighting the significant impact of CLD on daily functioning. This study underscores the need for effective disease management and improved patient outcomes.
The largest gland in the body, the liver, is found in the upper belly and weighs between 1 and 2,3 kg. It has four lobes: quad-rate, candidate, left, and right. The liver creates clotting factors, stores glycogen, detoxifies chemicals and processes nutrition. It is held up by peritoneal ligaments and encased in a thin capsule. Portal hypertension and liver dysfunction result from cirrhosis, a degenerative liver disease marked by regenerating nodules encircled by fibrous bands. It is brought on by chronic liver injury, which impairs liver function and blood flow. Varices, ascites, encephalopathy, and hepatocellular cancer are among the consequences that result from the disease's disruption of the liver's architecture. Common reasons include alcohol consumption, nonalcoholic fatty liver disease, and hepatitis C. The only treatment available is liver transplantation, though pharmaceuticals are being explored. (Heidelbaugh J, et.al., 2024)
Epidemiology: Alcoholic liver disease, hepatitis B/C, and non-alcoholic fatty liver disease (NAFLD) are common disorders that contribute to chronic liver disease (CLD), which is a major cause of death. About 41,500 people die from CLD each year in the United States, where it affects over 4.5 million adults
Risk factors: Alcohol consumption, nonalcoholic fatty liver disease (NAFLD), chronic viral hepatitis, autoimmune disorders, and genetic disorders such as hemochromatosis and alpha- 1 antitrypsin deficiency are the main causes of CLD. (Majid B, et.al.,2019)
Sign and symptoms: The most common sign and symptoms include ascites, portal hypertension, variceal bleeding, hepatic encephalopathy, jaundice, and coagulopathy. (Nezam H, et.al., 2024)
Management of chronic liver disease (CLD) involves a multifaceted approach targeting symptom relief, complications, and underlying causes. Anxiolytics like chlordiazepoxide are used to manage anxiety and agitation, particularly in cases of hepatic encephalopathy. Gastroprotective agents such as sucralfate mitigate gastric mucosal damage. Antivirals like tenofovir alafenamide address viral hepatitis when indicated. Beta-blockers, e.g., propranolol, are prescribed for portal hypertension to prevent variceal bleeding. Terlipressin, a vasopressor, is used for hepatorenal syndrome and variceal hemorrhage, while laxatives like lactulose reduce ammonia levels in hepatic encephalopathy. Diuretics such as spironolactone and furosemide help manage ascites, and albumin is administered for volume expansion and hypoalbuminemia. Hepatoprotective agents like ursodeoxycholic acid and ademetionine support liver function, while nutritional supplements like vitamin K and thiamine correct deficiencies. Antibiotics, including rifaximin and piperacillin-tazobactam, are used for infections like spontaneous bacterial peritonitis. (Dipiro JT, et.al., 2020) Health-related quality of life (HRQOL) is significantly impacted in patients with chronic liver diseases like cirrhosis. HRQOL can be assessed using tools like the SF-36, which evaluates physical and mental health, and the liver-specific Chronic Liver Disease Questionnaire (CLDQ), which focuses on symptoms like fatigue, abdominal discomfort, and emotional function. Higher scores on these tools indicate better quality of life. The Child- Pugh classification and MELD score help assess liver function severity, guiding treatment decisions and liver transplant eligibility. These measures aim to improve both survival and quality of life in patients with advanced liver disease. (Janani K et.al., 2018)
MATERIALS AND METODS:
Study site: -
The study will be conducted in St. Philomena’s Hospital, Bangalore
Study period: -
Study design: -
Inclusion criteria: -
Exclusion criteria: -
Patient with known case of Hepatocellular carcinoma.
Source of data: -
Method of study:
The research students will visit the Out-patient and In-patient wards of the hospital on a daily basis and enroll the patients as mentioned in the inclusion criteria. Informed consent will be obtained from each patient. All the demographics, social history, present complaints, past medical history, medication history, treatment pattern will be collected in the patient data collection form either from the prescription/patient case sheets. The Quality of Life of patients will be assessed by using Chronic Liver Disease Questionnaire (CLDQ). All the data collected will be pooled and analyzed.
Statistical Analysis:
A suitable statistical method will be employed based on the results.
Ethical Approval:
Ethical committee approval was obtained from the Institutional Ethics Committee of St. Philomena's Hospital, Bangalore.
RESULT AND DISCUSSION:
A total number of 102 Patients were enrolled from the gasterology OPD and IP of St. Philomena’s hospital
Our study revealed that a significant proportion of patients 74, (72.5%) were male. Similar trends have been observed in previous studies by Frith et al., The majority of patients 38 (37.3%) were between 51-60 years, followed by 23 (22.5%) patients aged 61-70 years. This is consistent with findings from Afdhal et al., who reported that CLD incidence peaks among middle-aged and elderly populations, primarily due to the cumulative impact of long-term alcohol use, viral infections, or metabolic disorders. In our cohort, 77 (75.5%) patients were managed as inpatients, and 25 (24.5%) required outpatient care. This aligns with research by Younossi et al., suggesting that most CLD cases, when identified early, can be managed with inpatient follow-ups unless complications like ascites or variceal bleeding arise.The study found that 65 (63.7%) patients had normal BMI, 25 (24.5%) were overweight, and 12 (11.8%) were obese outcomes in liver disease patients, as indicated by Kamila et al.. A majority 59, (57.8%) reported a history of alcohol consumption, with 12 (11.8%) having both alcohol and smoking habits. Alcohol use is recognized as one of the most common causes of CLD, consistent with the results of Banait et al., which emphasized that chronic alcohol consumption significantly contributes to cirrhosis-related hospitalizations and mortality. Seventy (68.6%) patients had pre-existing comorbid conditions, the most common being type 2 diabetes 17, (16.7%). The presence of diabetes in CLD patients is in line with findings from Maharani et al., who reported that metabolic disorders like diabetes increase the severity of liver disease and worsen outcomes. where 79(53.92%) alcohol consumption predominantly higher in men was highlighted as a major risk factor for liver disease. This gender discrepancy suggests the role of behavioral and lifestyle factors, including alcohol intake, as a dominant factor in the development of CLD shown in Figure 1 which was similar to result of Migbar Sib hat, et al, forty (39.2%) patients had 1-3 mg/dL total bilirubin levels, while 33 (32.4%) patients had 0.5-1 mg/dL direct bilirubin. Low albumin levels were found in 59 (57.8%) patients, indicating impaired liver function. These laboratory values reflect the typical presentation of CLD, where hypoalbuminemia and elevated liver enzymes are common. Fifty-nine (57.8%) patients had elevated AST levels (>40 U/L), and 49 (48.0%) had ALT levels above 35 U/L, indicating active liver damage. Additionally, 52 (51.0%) patients had prolonged prothrombin time (>14 sec), with the impaired synthetic function of the liver observed in cirrhosis cases, as noted by Ivanova Among patients undergoing ultrasound, 13 (12.7%) were found to have cirrhosis with mild hepatomegaly, while 12 (11.8%) had cirrhosis with splenomegaly. Procedures like endoscopic variceal ligation were not performed in 62 (60.8%) patients, and ascitic tapping was not required in 70 (68.6%) patients. where only patients with advanced disease or complications require invasive interventions. Nutritional management was a priority, with all patients in addition, 79 (77.5%) patients were on protein supplements and antibiotics, and 66 (64.7%) were prescribed diuretics. These interventions align with current guidelines recommending adequate protein intake and diuretics for patients with ascites, as which was similar to result of European Association for the Study of the Liver (EASL). Out of 102 patients, 89 (87.3%) showed improvement in their condition, while 6 (5.9%) patients unfortunately succumbed 7(6.86%)patients were Lama. These outcomes emphasize the importance of timely diagnosis and comprehensive management, as observed in other studies like Matos et al., which reported higher survival rates with early intervention. Using the SF-36 questionnaire, several aspects of HRQOL were evaluated. Sixty (58.8%) patients reported low energy or fatigue, indicating that fatigue is a prevalent and distressing symptom among CLD patients, Fifty-four (52.9%) patients had low physical functioning, reinforcing the idea that impaired physical capacity is common in chronic conditions like liver disease. Seventy-two (70.6%) reported bodily pain, underscoring the significant physical discomfort experienced by this population. Fifty-five (53.9%) patients reported average general health perception, showing a mix of physical and mental well-being concerns. Sixty-one (59.8%) patients had low physical role functioning, and 65 (63.7%) had low emotional role functioning, though 49 (48.0%) reported high social role functioning. Despite emotional challenges, these findings suggest that social support remained relatively intact. Additionally, 69 (67.6%) patients had low mental health scores, emphasizing the need for psychological interventions, which found that depression and anxiety are frequent comorbidities in liver disease patients. Overall, 61 (59.8%) patients had poor quality of life, 26 (25.5%) had moderate quality of life, and 1 (1.0%) patient reported good quality of life shown in Figure 2. With respect to gender, the majority of males (48, 47.1%) reported poor quality of life. In terms of age, the highest proportion (26, 25.5%) of patients with poor quality of life was in the 51-60 years group. Regarding social history, 49 (48.0%) alcoholics had poor quality of life. Among the 57 (55.9%) newly diagnosed CLD patients, 35 (34.3%) had poor quality of life, while 34 (33.3%) previously diagnosed patients also reported poor quality of life. In terms of age younger participants, especially those in the 20-40 age range, reported higher QoL scores, with all individuals in these age groups scoring between 85-100. In contrast, the older age groups exhibited progressively lower scores. Specifically, 65% of participants aged 51-60 scored in the 0-50 range, while those aged 61-70 and 71-80 had the lowest QoL, with 90.9% and 100% of individuals in these groups, respectively, scoring in the 0-50 range. This difference was statistically significant among this age (p>0.05). There was statistically significant difference in quality of life score between age group. Shown in Table 1, Our data is comparatively similar to a study conducted by Boehlen F et.al. The correlation of quality of life (QoL) scores with risk factors, significant findings were observed for diabetes mellitus (DM). Among participants with DM (n=52), a large proportion (73.1%) scored in the lowest QoL range (0-50), and this was statistically significant (p=0.003). There was statistically insignificant difference in Quality of life score between Diabetes mellitus (p<0 n=9), n=79),>0.05). This indicates that DM, HEPATITIS B, ALCOHOLIC, is strongly associated with a decline in QoL. Shown in Table 2, Among 102 patients the participants with a known case of CLD (n=60), a significant portion (65%) scored in the lowest QoL range (0-50), and only 6.7% scored in the highest range (85-100), with a new diagnosis of CLD (n=42), a more balanced distribution was observed 26.2% scored in both the highest (85-100) and intermediate ranges (51-84), while 47.6% were in the lowest range (0-50), There was statistically significant difference in quality of life score between Previously diagnosed and newly diagnosed (p<0>Table 3,Our data is comparatively similar to a study conducted by Paliogiannis P, et al.
CONCLUSION:
During the study period of nine months, a total number of 102 patients who met the inclusion criteria were recruited for the study from St. Philomena’s Hospital. This study revealed that a significant proportion of patients were male and majority of patients were between 51-60 years. It was observed that most of the patients had normal BMI with alcoholic history. The most common risk factor was alcoholic, hepatitisB and diabetes mellitus. Maximum patients were managed with protein supplements, antibiotics, diuretics and hepatoprotective agents respectively. SF-36 questionnaire revealed that majority of the patients had poor quality of life in terms of energy, physical function, body pain, General health perceptions, mental health, emotional role function, but in terms of social function majority of them had high quality of life. Overall, majority of the patients had poor quality of life, predominantly in males with the age group of 51-60 years, and they were mostly alcoholics. Mortality was observed in 6 patients, and 7 patients took LAMA, while 89 patients were improved and discharged. There was Statistical significance between age groups, risk factors such as alcohol and hepatitis B, patients with known case of CLD and quality of life There was Statistical insignificance between gender, risk factor such as Diabetes mellitus and quality of life. Hence, we conclude the study by stating that majority of the CLD patients were discharged from Hospital with one fourth mortality rate and majority of the patients had poor QOL which insists that proper counselling must be a part of Their hospital visit.
ACKNOWLEDGMENT
I would like to thank all the participants who had participate in the study. I acknowledge Al- Ameen College of Pharmacy and St. Philomena’s Hospital, Bangalore for providing me all the facilities to carry out the study.
REFERENCE
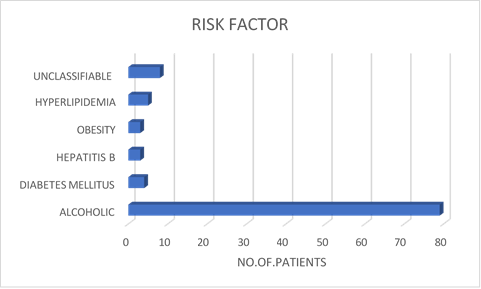
Figure 1 distribution of patients with respect to risk factors
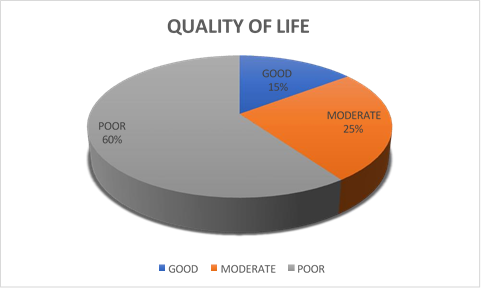
Figure 2 distribution of patients with respect to quality of life
Table 1 correlation of quality of life general value based on age and gender:
|
Variables |
general value |
P-value |
||
|
100-85 |
84-51 |
50-0 |
||
|
Gender |
|
|||
|
Male (n=78) |
11 (14.1%) |
21 (26.9%) |
46 (59%) |
0.910 |
|
Female (n=24) |
4 (16.7%) |
7 (29.2%) |
13 (54.2%) |
|
|
Age group |
|
|||
|
20-30 years (n=1) |
1 (100%) |
0 (0%) |
0 (0%) |
<0> |
|
31-40 years (n=6) |
6 (100%) |
0 (0%) |
0 (0%) |
|
|
41-50 years (n=22) |
8 (36.4%) |
12 (54.5%) |
2 (9.1%) |
|
|
51-60 years (n=40) |
0 (0%) |
14 (35%) |
26 (65%) |
|
|
61-70 years (n=22) |
0 (0%) |
2 (9.1%) |
20 (90.9%) |
|
|
71-80 years (n=11) |
0 (0%) |
0 (0%) |
11 (100%) |
|
Table 2 correlation of quality of life general value based on Risk factors:
|
variable |
General value |
P-Value |
||
|
|
100-85 |
84-51 |
50-0 |
|
|
DM |
|
|||
|
Yes (n=52) |
3 (5.8%) |
11 (21.2%) |
38 (73.1%) |
0.003 |
|
Hepatitis B |
|
|||
|
Yes (n=9) |
1 (11.1%) |
3 (33.3%) |
5 (55.6%) |
0.896 |
|
Alcoholic |
|
|||
|
Yes (n=79) |
12 (16.3%) |
21 (26.3%) |
46 (57.5%) |
0.669 |
Table 3 correlation of quality of life general value based on past history:
|
variable |
General value |
P-Value |
||
|
|
100-85 |
84-51 |
50-0 |
|
|
CLD |
|
|||
|
Known case (n=60) |
4 (6.7%) |
17 (28.3%) |
39 (65%) |
0.021 |
|
New case (n=42) |
11 (26.2%) |
11 (26.2%) |
20 (47.6%) |
|
Figure 1 distribution of patients with respect to risk factors
Figure 2 distribution of patients with respect to quality of life
Table 1 correlation of quality of life general value based on age and gender:
|
Variables |
general value |
P-value |
||
|
100-85 |
84-51 |
50-0 |
||
|
Gender |
|
|||
|
Male (n=78) |
11 (14.1%) |
21 (26.9%) |
46 (59%) |
0.910 |
|
Female (n=24) |
4 (16.7%) |
7 (29.2%) |
13 (54.2%) |
|
|
Age group |
|
|||
|
20-30 years (n=1) |
1 (100%) |
0 (0%) |
0 (0%) |
<0> |
|
31-40 years (n=6) |
6 (100%) |
0 (0%) |
0 (0%) |
|
|
41-50 years (n=22) |
8 (36.4%) |
12 (54.5%) |
2 (9.1%) |
|
|
51-60 years (n=40) |
0 (0%) |
14 (35%) |
26 (65%) |
|
|
61-70 years (n=22) |
0 (0%) |
2 (9.1%) |
20 (90.9%) |
|
|
71-80 years (n=11) |
0 (0%) |
0 (0%) |
11 (100%) |
|
Table 2 correlation of quality of life general value based on Risk factors:
|
variable |
General value |
P-Value |
||
|
|
100-85 |
84-51 |
50-0 |
|
|
DM |
|
|||
|
Yes (n=52) |
3 (5.8%) |
11 (21.2%) |
38 (73.1%) |
0.003 |
|
Hepatitis B |
|
|||
|
Yes (n=9) |
1 (11.1%) |
3 (33.3%) |
5 (55.6%) |
0.896 |
|
Alcoholic |
|
|||
|
Yes (n=79) |
12 (16.3%) |
21 (26.3%) |
46 (57.5%) |
0.669 |
Table 3 correlation of quality of life general value based on past history:
|
variable |
General value |
P-Value |
||
|
|
100-85 |
84-51 |
50-0 |
|
|
CLD |
|
|||
|
Known case (n=60) |
4 (6.7%) |
17 (28.3%) |
39 (65%) |
0.021 |
|
New case (n=42) |
11 (26.2%) |
11 (26.2%) |
20 (47.6%) |
|

Avinash S.*, Dr. T. Vithya, Dr. Praveen Kumar H. R., A Study on Assessment of Risk Factor, Management and Health Related Quality of Life in Cld Patients, Int. J. Sci. R. Tech., 2025, 2 (2), 96-101. https://doi.org/10.5281/zenodo.14846511
 10.5281/zenodo.14846511
10.5281/zenodo.14846511
